Overview
This case presents recurrent erosion of a Carlevale intraocular lens haptic following multiple previous repairs. The approach focuses on identifying the mechanical cause of repeated erosion and addressing it through scleral recession, patch grafting, and conjunctival reconstruction. The objective is to achieve stable coverage of the haptic in an eye with extensive prior surgery and limited conjunctival tissue.
Video on YouTube
Surgical management of recurrent Carlevale IOL haptic erosion using scleral recession, patch grafting and conjunctival autograft.
If age-restricted, please watch this video directly on YouTube.
Case context
- Prior surgery: The patient had a premium IOL exchanged for a monofocal lens, followed by retinal detachment requiring vitrectomy and Yamane fixation
- Scenario: The Yamane IOL subsequently dislocated and was replaced with a Carlevale IOL. The temporal haptic had eroded through conjunctiva and been patched four times, including with donor cornea, while the nasal haptic remained stable
- Focus of video: This was the fourth IOL in the eye, and further IOL exchange was not desirable
Key observations
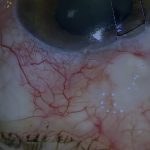
- The eroding haptic was positioned proud of the scleral surface, unlike the contralateral haptic which was flush
- Repeated conjunctival breakdown occurred despite multiple prior patch grafts
- Scleral grooving and cautery were used to recess the haptic into sclera
- A corneoscleral patch graft was placed with its anterior edge buried in a corneal groove
- Limited conjunctival mobility required a conjunctival autograft from the inferior fornix
Transcript
I am referred some very interesting and unusual cases that have nothing to do with glaucoma. These vary from cyclodialysis clefts to patients with thin sclera, but the patient I am going to present here was particularly interesting because it was a case of a Carlevale haptic erosion that had been patched several times and was threatening to erode again.
The challenge I faced with this case was that I was not sure that I could do any better than the previous surgeons, so I had to think very carefully about what was causing the erosion and how it could be prevented from happening again.
Read more
In this video I am going to describe how I approached the repair of a rather unusual Carlevale intraocular lens haptic erosion.
This patient had a premium IOL replaced with a monofocal due to dissatisfaction with the visual outcome. Subsequently, the retina detached, requiring vitrectomy with a Yamane-type IOL fixation. The Yamane IOL then dislocated and was replaced with the Carlevale IOL.
The temporal haptic of the Carlevale IOL subsequently eroded through conjunctiva and had been patched on four separate occasions, and looked as if it was about to erode again despite having been patched multiple times, even with donor cornea.
As this is the fourth IOL in this eye and the patient is pleased with the vision, a further IOL exchange is not desirable. The nasal haptic has been fine so far.
So how do I prevent this haptic from eroding again?
I was not sure exactly how to prevent further erosion, but the first step was to explore and assess.
This temporal conjunctiva has been opened six previous times, so careful dissection is required. The area around the haptic is gently de-epithelialised.
The conjunctiva is very tight from multiple previous operations and will need to be mobilised extensively for later closure. This buttonhole is likely to be the least of my problems when attempting closure later.
Why has this haptic eroded repetitively while the other has not?
This haptic seems almost flush with the scleral surface, while this haptic is clearly sitting proud above the scleral surface.
An obvious approach is to try and recess the haptic into sclera.
I attempt to achieve this by grooving the sclera with a blade under the haptic. This will only be feasible if the underlying sclera is of adequate thickness.
Cautery is then applied inside the groove to shrink the tissue. These actions are performed repetitively until the haptic is adequately recessed in sclera.
A 10-0 nylon mattress suture is then used to compress the haptic into the groove to render it as flush as possible with sclera.
Although most of the haptic is now recessed, the superior end is still sitting proud, so further grooving is required. The end of the haptic now appears to be better recessed.
The next step is to cut a corneoscleral patch to cover the haptic.
To cover the haptic adequately, the patch must be as close to the limbus as possible to avoid a large step at the limbal edge of the patch. The anterior edge will be buried in a peripheral corneal groove.
Persistence is required as the groove needs to accommodate the anterior edge of the corneoscleral patch graft.
To minimise the risk of yet another haptic erosion, the ocular surface over the haptic must be as smooth as possible.
The front edge of the patch is sutured with 10-0 nylon in a manner that pulls it into the groove. Fibrin glue is applied underneath the patch to stabilise it. Additional sutures are added to compress the back of the patch against the patient’s sclera.
Because this is the fourth IOL in this eye and it has eroded so often, I am using belt-and-braces techniques to prevent further erosion.
Further conjunctival mobilisation is attempted before closure, but it is not enough because there has been so much previous surgery.
A conjunctival autograft will be required for closure, but due to the amount of previous surgery there is very little mobile conjunctiva available.
The defect is carefully measured and minimised. The conjunctiva to be harvested from the inferior fornix is then measured and marked with cautery.
When patching erosions I would often incorporate a thick layer of Tenon’s when harvesting the autograft. In this case, due to a shortage of tissue in the inferior fornix, I largely only harvested conjunctiva for the autograft.
The autograft is then transferred to the recipient site, taking care to maintain the orientation, keeping the epithelial side up.
The autograft is anchored with fibrin glue before suturing. The glue prevents the autograft from sliding or rolling while it is being sutured.
The autograft is sutured in place with a locked continuous Tenon’s suture, in this case nylon. The locked continuous suture is tied off intermittently.
The conjunctiva is also secured tightly at the limbus.
Four weeks after surgery the ocular surface is still settling and the conjunctival sutures are still in place. The haptic is still well covered and although these are early days, so far there is no indication that the haptic will erode again.
For outcome benchmarking, see the International Glaucoma Surgery Registry.