Overview
Paul implant overdrainage management requires careful titration of ligature tension when a fully inserted rip cord does not sufficiently restrict aqueous drainage. This video demonstrates intraoperative identification of excessive flow and adjustment using 10-0 nylon ligature. It emphasises variability between implants and the need for real-time flow assessment. The approach focuses on achieving physiological drainage while avoiding both hypotony and excessive IOP.
Video On YouTube
Intraoperative management of overdrainage in a Paul glaucoma implant using adjustable ligature technique.

If age-restricted, please watch this video directly on YouTube.
Case Context
- Prior surgery: Paul glaucoma implant insertion
- Scenario: Intraoperative overdrainage despite full rip cord insertion
- Focus of video: Adjustment of aqueous outflow using 10-0 nylon ligature to achieve controlled drainage
Key Observations
- Manufacturing variability in implants and rip cords affects drainage behaviour [00:31]
- Clear visualisation of the aqueous exit point is required to accurately assess flow [02:08]
- Fluorescein may be limited, while Vision Blue improves visualisation of drainage [03:19]
- Initial three throws of 10-0 nylon ligature are used to titrate flow before locking [04:33]
- Over-tight ligation risks high postoperative IOP, while under-correction risks hypotony [08:54]
Transcript
[00:00] I’m recording this video from the American Academy of Ophthalmology annual congress in Orlando. Last year, I posted a video on what to do if a Paul glaucoma implant failed to drain intraoperatively on the table.
The subject of the video I’m showing today is the opposite. What if it drains too much?
Read Full Transcript
We are becoming increasingly used to using all sorts of implants in glaucoma to lower the intraocular pressure. An important point however is to understand that these all vary slightly from batch to batch. This is true of the Paul glaucoma implant, was true of the Baerveldt, was true of the Ahmed glaucoma valve, and is true of pressure-flow microshunts such as XEN.
Every implant that we use has some manufacturing variability, and indeed if we also occlude these with intraluminal rip cords, the rip cords also have variability. We therefore cannot expect one size to fit all and we must be prepared to look at the amount of drainage that we’re getting and adjust as necessary.
In this video, I’m going to show how to adjust if the drainage is too much on the table.
Identifying Overdrainage and Initial Management Approach
In this video I’m going to describe what I do if a Paul glaucoma implant is overdraining intraoperatively after the rip cord has been fully inserted.
This Paul glaucoma implant is clearly draining too briskly even though the rip cord is the whole way along the tube. A 10-0 nylon ligature is often the best option in this situation, offering some constriction while being easy to laser in clinic later.
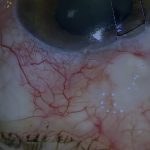
While the requirement for ligature in this eye is clear-cut, the answer is not always quite so obvious. When checking the drainage from a Paul or Baerveldt implant, it is essential to keep Tenon’s clear of the aqueous exit point. Otherwise, the surgeon cannot be sure of what is going on.
Here visualisation is poor. When conjunctiva and Tenon’s are lifted clear of the aqueous exit point, the brisk flow becomes much more obvious.
7-0 silk traction sutures in the Tenon’s are extremely helpful in improving visibility when suturing and checking drainage. They retract Tenon’s and prolapse the globe slightly. They also keep stray lashes away from the PGI plate and greatly improve visualisation of the aqueous drainage.
Assessing Flow and Use of Adjuncts
Sometimes despite traction sutures, access is still difficult, so I use fluorescein in an attempt to estimate the flow. However, fluorescein by itself often doesn’t help much.
On the other hand, Vision Blue, either in isolation or mixed with fluorescein, offers better visualisation of the drainage.
If the well is clearly seen to be filling up rapidly, or if a droplet develops rapidly outside the well, and the rip cord has been fed along the whole length of the tube into the anterior chamber, then the next step is to ligate the tube.
Many surgeons use an absorbable ligature such as Vicryl, but this has a disadvantage of lack of control over release timing. My standard ligation technique is to use 10-0 nylon sutures tensioned to reduce but not eliminate drainage completely.
Ligature Technique and Intraoperative Adjustment
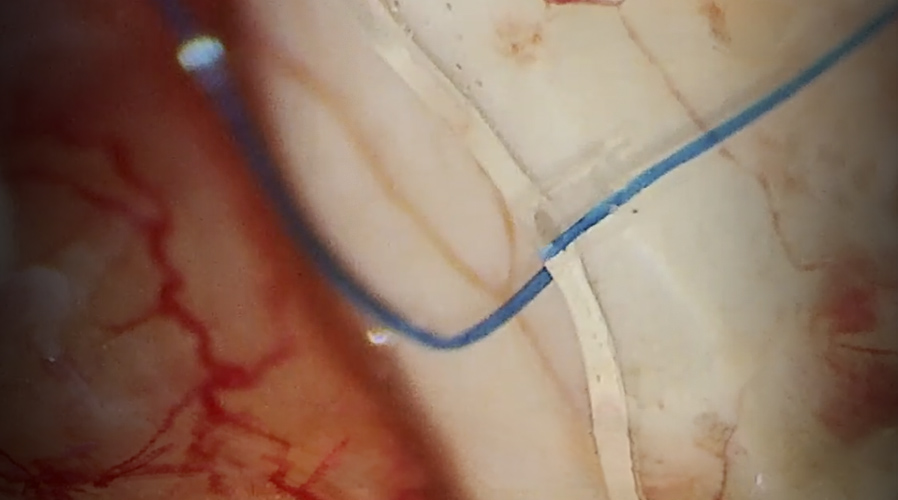
This PGI is draining too quickly although the rip cord has already been fed all the way into the anterior chamber. A 10-0 nylon ligature will therefore be applied to the tube in addition to the rip cord.
Three throws are applied initially and the flow rechecked. The anterior chamber is pressurised and the flow retested. The rate of drainage is now acceptable.
If the flow is acceptable with the initial three throws, the knot is gently locked, avoiding further constriction of the ligature. It is essential to avoid locking down tightly as further constriction will eliminate flow, resulting in a high postoperative IOP.
The knot is therefore locked down gently so the ligature is not tightened further. If the knot is inadvertently overtightened, it can often be loosened slightly by wiggling and stretching with forceps.
In this case, I’m gluing a fascia patch graft to sclera, ensuring that the limbal edge of the tube is well covered. When patching the tube, it is important not to cover the ligature as it must be visible to laser postoperatively if required.
Fine-Tuning Ligature Tension
Back to the initial case that I showed at the start of this video. Again, I put three throws on a 10-0 nylon without locking it. On checking the flow, this seems to be a little too tight.
At this stage, it is easy to loosen the three throws slightly, increasing the flow rate again. The rate of drainage is now a little too brisk, so I tighten the ligature again slightly without locking it down. The rate of drainage is now acceptable.
The 10-0 nylon ligature is then locked down gently, trying to avoid constricting the tube further. After pressurising the eye, it seems that the constriction is not quite enough after all, so I tighten the previous throw, increasing the constriction.
The drainage is now significantly less than before.
Managing Resistant Overdrainage and Escalation
This PGI is also draining briskly. As with the previous cases, I aim to reduce aqueous flow to a physiological level with the initial three throws before locking. This results in a promising reduction in aqueous flow.
However, it is important at this stage to ensure that the anterior chamber is adequately pressurised. Pressurising the anterior chamber has dramatically increased the drainage in this eye despite the partially secured ligature.
So I tighten the ligature again, still only with the initial three throws without locking it down. But this is still not enough, so I tighten the ligature a little more.
But the rate of drainage has barely reduced. Here the initial three throws have not been enough to reduce the flow to a physiological rate, so I proceed to lock the knot, adding a little more tension to the ligature as I lock down the suture while avoiding tightening it too much.
The rate of drainage is now at the upper end of acceptability, but a little too much if there are risk factors for hypotony. If this patient were at high risk of hypotony or complications should hypotony occur, I would add another ligature.
On close inspection, the ligature can be seen to be constricting the tube quite significantly.
Key Principles and Avoiding Overcorrection
The key point is that if a Paul glaucoma implant is draining too quickly when the rip cord is all the way in, a single adjunctive ligature should not be a crude all-or-nothing tool with a binary outcome, but should be adjusted according to the rate of drainage when the anterior chamber is adequately pressurised.
This permits a physiological rate of drainage and appropriate postoperative IOP immediately after surgery, so that patients with advanced glaucoma do not lose vision from hypotony or from high IOP in the early postoperative period.
It is important not just to avoid hypotony but also to avoid overcompensating for the risk of hypotony. In the past, it has been common practice to ligate tubes very tightly to prevent hypotony. This then results in a very high pressure and sometimes leads to the surgeon releasing the ligature in order to prevent the high pressure, thereby causing hypotony again.
The primary aim at the time of surgery is not just to avoid hypotony, but to avoid overcompensating for the risk of hypotony.
For outcome benchmarking, see the International Glaucoma Surgery Registry.