Overview
XEN bleb excision glaucoma implant surgery is performed to remove a dysaesthetic overhanging bleb and convert to a Paul Glaucoma Implant. The procedure demonstrates staged implantation to maintain globe firmness during surgery. Tube positioning, flow control, and bleb excision are shown sequentially. Management of the XEN entry site and conjunctival closure are also demonstrated.
Video On YouTube
This video demonstrates XEN bleb excision with conversion to a Paul Glaucoma Implant.

If age-restricted, please watch this video directly on YouTube.
Case Context
- Prior surgery: XEN gel implant
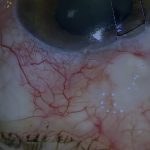
- Scenario: Dysaesthetic overhanging bleb requiring removal
- Focus of video: Bleb excision with simultaneous Paul Glaucoma Implant insertion
Key Observations
- Paul Glaucoma Implant inserted before bleb excision to maintain globe firmness [00:03]
- Plate secured with diagonal 9-0 polypropylene sutures to minimise movement [00:47]
- Tube length adjusted after identifying excess length in anterior chamber [01:38]
- Bleb capsule opened from behind and amputated to expose and remove XEN [02:09]
- Fascia lata used to plug persistent drainage at XEN entry site with tissue glue [03:12]
Transcript
I’m going to demonstrate how I dealt with a dysaesthetic overhanging XEN gel implant bleb without losing pressure control.
This patient had a very dysaesthetic overhanging XEN bleb. To fix the dysaesthetic bleb, the XEN will also be removed and a Paul Glaucoma Implant inserted. The Paul is implanted before excising the bleb so that the globe remains firm during implantation.
Read Full Transcript
Case Overview And Surgical Plan
0.5 mg per ml of MMC is applied on sponges to the undersurface of the equatorial Tenon’s for 5 minutes prior to implanting the PGI plate. This is not shown here.
Plate Fixation And Tube Insertion
The plate is secured with two 9-0 polypropylene sutures orientated diagonally to minimise lateral plate movement and anteroposterior plate movement.
The anterior chamber is entered just anterior and parallel to the iris plane with a 25-gauge needle.
The tube is secured with two 9-0 nylon mattress sutures, each with two-point fixation to sclera, minimising movement. Nylon rather than Prolene is used. The tube knots are buried away from the tube to minimise the risk of erosion.
Tube Positioning And Flow Assessment
The aqueous exit point over the plate is then checked to ensure that drainage is adequate but not excessive.
At this point the tube is noted to be too long in the anterior chamber, so it is trimmed and reinserted. The anterior chamber is pressurised again with balanced salt solution before rechecking the drainage.
Once a satisfactory rate of drainage has been confirmed, the XEN bleb and the XEN need to be dealt with.
Bleb Excision And XEN Removal
The bleb capsule is entered from behind and the roof of the capsule flipped forward, exposing the XEN.
The capsule is then amputated. Next, the remaining portion of the bleb overhanging the cornea is identified and also amputated.
The XEN is then removed gently, as these implants are very fragile, and you can see a small portion is broken off.
Paul Glaucoma Implant Completion And XEN Site Management
A partial-thickness limbal groove is fashioned to accommodate the corneal loop of the 6-0 Prolene intraluminal occluding suture in the Paul Glaucoma Implant.
The XEN entry site is still draining and is resistant to hydration with BSS using a 30-gauge Rycroft cannula.
A small sliver of fascia lata is cut from the patch graft that will be applied over the Paul Glaucoma Implant tube. The thinly tapered end of the fascia is inserted into the draining XEN tunnel, plugging it. The fascial plug is then glued in place using tissue glue.
Fluorescein confirms there is no further drainage. The XEN entry site and the Paul Glaucoma Implant tube are both covered by a larger fascia lata patch graft than usual in order to encompass both entry sites. The fascial patch graft is secured with tissue glue.
Conjunctival Closure And Key Considerations
In general, if a large bleb is excised in combination with tube implantation, extensive conjunctival mobilisation is required before closure.
In this situation tissue glue is helpful but not enough to secure conjunctiva without additional suturing. The conjunctiva is then secured using multiple locked Tenon’s nylon continuous sutures.
For outcome benchmarking, see the International Glaucoma Surgery Registry.