Overview
This case demonstrates the removal of a Hydrus Microstent implanted nine years earlier that had become malpositioned and caused progressive corneal oedema. Gonioscopy suggested a suprachoroidal position, but intraoperative findings revealed entrapment within the peripheral iris stroma. The video outlines the failed Sinskey hook approach and subsequent use of micro-graspers and 23-gauge scissors to achieve safe explantation with minimal visible trauma.
Video on YouTube
Hydrus Microstent removal is shown in this case of late malposition with corneal oedema and intraoperative iris stroma entrapment.

If age-restricted, please watch this video directly on YouTube.
Key points
- Malpositioned Hydrus Microstent identified nine years post-implantation, causing endothelial compromise.
- Initial assumption of suprachoroidal placement proved incorrect; the device was embedded in the iris stroma.
- Attempted removal with a Sinskey hook was unsuccessful due to lack of accessible windows.
- Micro-graspers and 23-gauge scissors enabled controlled dissection and removal with limited iris trauma.
- Post-operative review showed reduced corneal clarity but minimal angle damage, with endothelial keratoplasty anticipated.
Transcript
Hydrus Microstent Removal: Iris Stroma Entrapment
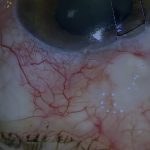
This case involves a patient with a Hydrus Microstent implanted nine years earlier, which had begun to cause problems. The issue was not due to the device being correctly positioned—it was due to it being in the wrong place. From the appearance, I initially thought it was in the suprachoroidal space, but this turned out not to be the case.
The Hydrus could be seen protruding into the anterior chamber beneath the trabecular meshwork eight weeks after insertion, around nine years ago. On gonioscopy, the appearance was suggestive of suprachoroidal rather than Schlemm’s canal placement. [01:00]
Read more
A Hydrus Microstent implanted nine years earlier was found to be malpositioned and causing progressive corneal oedema. Gonioscopy initially suggested a suprachoroidal location, but intraoperative findings revealed the device trapped in the peripheral iris stroma. After unsuccessful attempts with a Sinskey hook, careful dissection with 23-gauge scissors allowed safe removal. Post-operatively, the angle showed minimal visible trauma, though endothelial keratoplasty may be required to restore clarity.
Progressive Corneal Changes and Decision to Remove
Four to five years later, in 2024, the visual acuity had gradually reduced to 6/60 in the eye implanted in 2015. There was significant corneal oedema, and the central corneal endothelial density was reduced to 875 cells/mm² compared with 1,537 in the fellow eye. The malpositioned Hydrus was suspected to be compromising the endothelial cell count and causing chronic discomfort. The decision was therefore taken to attempt removal of the malpositioned Hydrus Microstent. [02:40]
Attempted Removal with Sinskey Hook
I first attempted to engage the Hydrus using a Sinskey hook. However, one Hydrus window needs to be accessible for the Sinskey hook to be effective. There was no such accessible window in this case. While a Sinskey hook can easily be inserted into the Hydrus window, it cannot be used to engage the flanges or the slot on the Hydrus inlet. [03:00]
Use of Micro-Graspers and Dissection Technique
Instead, I used micro-graspers to gently tease the Hydrus circumferentially, avoiding radial movements that might cause disinsertion. The first window of the Hydrus became free, though the rest of the implant remained tethered to the tissues. After another attempt to release the remainder, it became clear that the device would not shift. Rather than being in the suprachoroidal space as originally assumed, the Hydrus appeared to be trapped within the peripheral iris stroma. Consequently, the implant was freed by gently dissecting the anterior iris stroma using 23-gauge vitrectomy scissors. [04:00]
Removal Outcome and Post-Operative Appearance
Eventually, the Hydrus was completely freed and removed from the anterior chamber. The viscoelastic was then removed, and the wounds were hydrated. Four weeks after surgery, some angle and peripheral iris details could still be seen through the residual corneal oedema. The angle and iris appeared to have sustained far less visible trauma than anticipated. However, the patient is still likely to require endothelial keratoplasty to restore corneal clarity. [05:00]
Closing Comment
I hope you found this video useful, and I also hope you never have to remove a Hydrus from the iris stroma or suprachoroidal space, as these are potentially hazardous procedures.
For outcome benchmarking, see the International Glaucoma Surgery Registry.