Overview
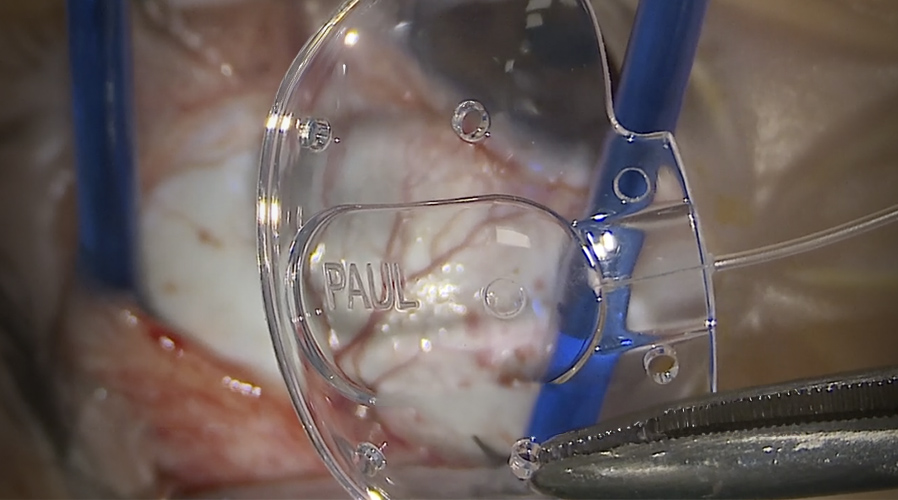
The Paul Glaucoma Implant can achieve more stable physiological pressures in the early post-operative period, but occasionally the device may not drain visibly at the time of surgery. This video demonstrates practical intraoperative steps for restoring flow, including confirming adequate intraocular pressure, controlled flushing, and adjusting the ripcord. It also highlights situations in which switching from 6-0 to 7-0 Prolene or widening the entry tract may be necessary.
Video on YouTube
The Paul Glaucoma Implant can provide predictable early pressure control, but occasionally requires intraoperative drainage troubleshooting, find out more in the video, or read on below.

If age-restricted, please watch this video directly on YouTube.
Key points
- Confirm adequate intraocular pressure before assessing drainage.
- Flush the tube repeatedly, ideally from the plate end, to re-establish flow.
- Check the ripcord end for a clean bevel to avoid mechanical obstruction.
- Switch to 7-0 Prolene when 6-0 is too tight to allow safe, consistent flow.
- Consider a tight anterior chamber entry tract if patency and flushing are normal.
Transcript
Over the last 20 years, I have been a high-volume user of aqueous shunts or glaucoma drainage devices, specifically the Baerveldt implant, because of broad efficacy in a wide variety of extremely challenging cases. In the last six years, I have switched completely to the Paul Glaucoma Implant, because of the ability to obtain more predictable physiological pressures in the early post-operative period, with similar long-term efficacy. This has made life a lot easier. However, as with all devices, there is a degree of variability, and we cannot expect exactly the same results in every patient without occasional adjustments in technique.
Restoring Drainage in the Paul Glaucoma Implant
One particularly frustrating problem can be difficulty obtaining visible drainage from the back of the tube on the table after what appears to be a normal implantation with a 6-0 polypropylene ripcord. Sometimes, even with progressive withdrawal of the ripcord, and even when the 6-0 Prolene is completely removed with the tube in the anterior chamber, there is still no drainage.
Read more
{{EXTENDED_NOTES}}
Ensuring Adequate Intraocular Pressure and Flushing
The first step is to ensure the eye is adequately pressurised. If there is still no drainage, I flush the tube using a 30-gauge Rycroft cannula. If there is still no drainage, I repeat the flush, this time with a prolonged flush. This generally leads to success. I then reinsert the Prolene quickly to avoid prolonged ocular decompression. Drainage may now be visible, though sometimes only a very short length of the 6-0 Prolene remains in the tube.
When 6-0 Prolene Is Too Tight
Occasionally, 6-0 Prolene will be too tight to permit drainage even when only a very small length is in the tube. It is useful to check that there is no bulb on the cut end of the suture. If the cut was not clean, the end may be slightly bulbous and obstruct the tube. I aim for a clean, slightly bevelled cut so the suture inserts more easily.
In another example, despite a clean bevelled cut, there was still no drainage until less than 1 mm of ripcord remained, which risks the suture falling out later.
Switching to 7-0 Prolene
The solution is to swap the 6-0 Prolene for 7-0 Prolene. The difference in gauge produces lower resistance, so the 7-0 must be threaded further up the tube. Drainage then becomes slightly brisk but not excessive.
If the Implant Still Does Not Drain
If drainage still does not occur despite repeated flushing, check tube patency in the anterior chamber and ensure it is not occluded with iris or blood. If necessary, remove the tube from the anterior chamber and flush again from the distal end using a 21- or 20-gauge cannula. Assess how much of the lumen the ripcord fills; if no gap is visible, the ripcord is probably too tight.
Cannula Choice
A 20-gauge cannula is effective; a 21-gauge fits more tightly and reduces leakage. A 23-gauge can be used from the plate end. A 27-gauge cannula fits precisely into the plate well and flushes with the least effort.
Tight Entry Tract
In rare cases, a tight anterior chamber entry tract may compress the tube. Gently widening the entry site, for example with a 30-gauge Rycroft cannula, may resolve the problem. The Prolene can then be rethreaded and flow rechecked.
For outcome benchmarking, see the International Glaucoma Surgery Registry.