Overview
The Preserflo MicroShunt provides a subconjunctival drainage approach with a relatively predictable post-operative course when patient selection and surgical detail are carefully considered. This discussion focuses on how pre-operative factors, mitomycin-C handling, device positioning, and early flow control influence bleb morphology and intraocular pressure stability. Practical steps to reduce hypotony risk, including intraluminal stenting with a removable ripcord, are demonstrated and explained for routine surgical use.
Video on YouTube
Preserflo MicroShunt implantation benefits from careful case selection, MMC handling and early flow control to support predictable bleb formation.
🔞 This video is age-restricted. Please watch it on YouTube.
Key points
- Choose patients likely to do well with a subconjunctival drainage approach; avoid cases where a trabeculectomy would predictably fail.
- Use a large peritomy and controlled mitomycin-C placement to support diffuse posterior bleb formation.
- Ensure a single clean anterior chamber entry and stable device seating to maintain ideal positioning.
- Consider intraluminal ripcord stenting in patients at risk of early hypotony, particularly elderly individuals.
- When bleb failure occurs, evaluate carefully whether revision or conversion to a tube is the more appropriate next step.
Transcript
Preserflo MicroShunt Surgical Technique
The introduction of the Preserflo MicroShunt has made a significant contribution to my glaucoma surgical practice. In this presentation, I will outline my approach to pre-operative case selection, nuances in surgical technique and aspects of post-operative care. I hope you find it useful and interesting.
I have a number of financial disclosures, as I work with many companies. I do not have a specific financial interest in the Preserflo MicroShunt, but I have served on advisory boards for Santen and have received speaker honoraria and travel expenses.
Read more
This presentation outlines patient selection criteria, surgical technique and post-operative management for the Preserflo MicroShunt. Key considerations include choosing patients likely to benefit from a subconjunctival drainage approach, meticulous control of mitomycin-C exposure and awareness of risk factors for hypotony. Temporary intraluminal stenting with a ripcord suture provides an effective strategy for reducing early over-drainage in selected cases.
Device Overview and Bleb Characteristics
The Preserflo MicroShunt is a small polymer tube that drains aqueous humour from the anterior chamber to the subconjunctival space, similar in principle to a trabeculectomy. However, insertion is simpler and the post-operative care is generally less intensive. The device consists of a 3 mm subconjunctival portion exiting approximately 3 mm behind the limbus, a 1.1 mm scleral fin for self-retention, and a 5 mm intraocular portion. Post-operative bleb morphology is typically more posterior and diffuse, although higher doses of mitomycin-C are often required compared with trabeculectomy.
Case Selection Considerations
Case selection is important. I avoid the Preserflo MicroShunt in patients in whom I would not expect a trabeculectomy to function well, including those with significant conjunctival scarring, certain secondary glaucomas, previous vitrectomy with silicone oil and neovascular glaucoma. Subconjunctival MIGS procedures may be more challenging in higher-scarring ethnic groups, and failure rates may be higher.
Surgical Technique Walkthrough
The conjunctival and Tenon’s dissection is similar to a trabeculectomy, but implantation does not need to be centred at 12 o’clock. A slightly temporal peritomy is often preferable. Thorough haemostasis is essential, and mitomycin-C sponges are placed posteriorly for approximately 3 minutes. A 3 mm posterior scleral mark is created and a 1 mm-wide tunnel fashioned. A bent 25-gauge needle is used to enter the anterior chamber just anterior to the iris. The Preserflo MicroShunt is inserted bevel-up and allowed to self-retain. If flow is not visualised, balanced salt solution flushing via a thin-walled cannula may establish drainage. During closure, avoid obstructing the device with Tenon’s tissue.
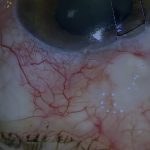
Post-Operative Course and Bleb Appearance
At around one week, the bleb is often red but functioning, with controlled pressure. Several months later, blebs are usually quiet and diffuse.
Hypotony Risk and Ripcord Stenting Technique
Occasional cases of severe post-operative hypotony were observed, particularly in older patients. To reduce this risk, I may reduce mitomycin-C exposure and insert an intraluminal ripcord, typically 9-0 polypropylene or 10-0 nylon. A corneal groove allows later removal at the slit lamp, and a scleral bite helps prevent device displacement. The suture is adjusted to balance flow and usually removed after three to four weeks.
Management of Preserflo Failure
If pressure rises and the bleb is flat, I assess device patency. Needling is often ineffective if peri-tubular fibrosis has developed. In such cases, I may re-open the conjunctiva, reapply mitomycin-C and remove scar tissue, replacing the device if flow is inadequate. Success of revision is generally lower than primary implantation, and in some cases proceeding to a tube may be preferable.
Closing Note
The Preserflo MicroShunt is a valuable part of my practice when used selectively. I hope these considerations are useful.
For outcome benchmarking, see the International Glaucoma Surgery Registry.