Overview
This video demonstrates scleral leak repair for severe hypotony, initially suspected to be a cyclodialysis cleft, and an anterior chamber lens exchange to an Artisan iris-fixated IOL. It shows the decision pathway from inconclusive UBM through targeted exploration under scleromalacia, intraoperative leak confirmation, and corneoscleral patch placement under tension. Practical steps for exposure, patch fixation, and enclavation are shown, with early postoperative outcomes relevant to surgical planning and risk reduction.
Video on YouTube
The video demonstrates hypotony repair following a scleral leak under scleromalacia with corneoscleral patch and lens exchange.

If age-restricted, please watch this video directly on YouTube.
Key points
- Consider scleromalacia leak as a cause of hypotony in rare situations where there is significant angle recession under the scleromalacia and no other cause of the hypotony can be found.
- Use viscoelastic-filled gonioscopy (e.g. Ahmed gonioprism) to reassess suspicious angle recession.
- Tailor a corneoscleral patch to the limbal curvature and secure it under tension for watertight closure.
- Stabilise optics by exchanging a mobile AC IOL to an Artisan lens with careful iris enclavation.
- Pressurise and recheck for posterior edge leakage before conjunctival closure with fibrin glue.
Transcript
Hypotony Repair Following Scleromalacia Leak
Introduction. I’m frequently referred patients with hypotony who are suspected of having a cyclodialysis cleft, as I have a particular interest in cyclodialysis cleft repair. I can usually predict from the history whether there is a high likelihood of a cleft. However, in this case, I was mistaken — it turned out to be something completely different.
Clinical Background. This patient was referred with a wobbly anterior chamber intraocular lens, scleral thinning, and hypotony. Clinically, the patient displayed the ophthalmic and cardiac features of Marfan syndrome, but without the fibrillin gene mutation. While scleromalacia is not typical of Marfan syndrome, there had been spontaneous lens dislocation in both eyes and a heart valve replacement.
Read more
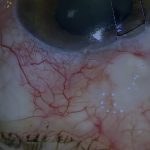
On gonioscopy, there appeared to be an area of angle recession and possibly a cyclodialysis cleft under the area of scleromalacia. [01:15]
Imaging And Initial Impression
Although this area looked very suspicious for a cleft, no definite cleft was seen on ultrasound biomicroscopy (UBM), even after anterior chamber injection of viscoelastic. Surgical exploration was therefore required to diagnose and treat the hypotony if possible, and to exchange the intraocular lens.
Gonioscopy was first repeated after filling the chamber completely with viscoelastic and using the Ahmed gonioprism. The same suspicious area was visualised more clearly, but there was still no definitive sign of a cyclodialysis cleft. [02:00]
Despite this, the eye had severe, unexplained hypotony, and the area of recession likely harboured a cleft.
Surgical Exploration
The suspicious area lay under the scleromalacia, so exploration began there. As the conjunctiva was opened, the choroid or ciliary body appeared to be prolapsing through the scleromalacic area. [02:40]
This type of prolapse is not particularly unusual when opening conjunctiva over areas of scleromalacia and usually requires patching before closure. However, this finding was unexpected. I had not previously seen fluid leaking from areas of scleromalacia.
To determine whether the drainage was from the anterior chamber or the suprachoroidal space, Vision Blue was injected. Although subtle, there was some blue staining of the draining fluid, which did not completely exclude a suprachoroidal origin if a cleft were present.
However, as the leak was over an area of deep angle recession, it most likely originated from the anterior chamber, making a cleft unnecessary to explain the hypotony. The leaking scleromalacia was therefore considered the cause. The leaking area was approximately 3.5 mm from the limbus.
Repairing The Scleromalacia
In situations like this, I like to use 7-0 silk sutures to retract Tenon’s capsule to maximise exposure of the area. These sutures also slightly prolapse the globe, improving access.
A patch of human donor cornea or corneoscleral ring was used to seal the leak. As the area of scleromalacia was circumferential, a segment from the same part of the donor eye was chosen to fit best, but the first segment was too short. A longer segment was therefore cut and tailored to fit the curvature of the limbus and to cover the full area of scleromalacia.
The donor sclera was initially fixed in place with fibrin glue. To ensure a watertight seal, the donor patch was then secured under tension against the host sclera. The limbal portion was sutured especially tightly to minimise the risk of post-operative leakage. [06:40]
Intraocular Lens Exchange
The next step was to address the problem of the very mobile anterior chamber intraocular lens. The lens was rotated to facilitate removal, and a mushroom hook was used to engage the haptic. [07:35]
Small stab incisions were made on either side of the main wound using a 23-gauge MVR blade. The Artisan lens that would replace the previous anterior chamber lens was then inserted and dialled horizontally.
After partial closure of the main wound, the peripheral iris was enclaved in the gap in the haptic using a needle and micro-graspers. Once the first haptic was secure, the same was performed for the second.
The lens was initially decentered, and the first haptic may have freed itself from the iris. It was therefore repositioned and re-enclaved using the micro-graspers and needle. When the intraocular lens was stable and centred, and all viscoelastic had been removed, the wound was closed. [10:00]
Closure And Post-Operative Outcome
Once the corneal wound was watertight, the back of the scleral patch was secured with 10-0 nylon sutures at the site of the leak. The patch was then tightened over normal sclera, and the anterior chamber was pressurised with balanced salt solution. The posterior edge of the patch was checked for leakage and appeared watertight. The conjunctiva and Tenon’s were closed with fibrin glue.
Fifteen days later, the eye was settling, with a stable intraocular lens, quiet anterior chamber, normal intraocular pressure, and improving visual acuity. [12:40]
One month after surgery, there was some minor conjunctival recession, not of clinical significance. Eight weeks post-operatively, visual acuity was 6/9.5 unaided, pressure was 9 mmHg without medication, and the intraocular lens remained stable.
Reflections
This case turned out to be unusual — I have never previously seen hypotony caused purely by leakage through scleromalacia. The patient was recovering well post-operatively, though it was still early days. I would also like to thank my colleague, Vincenzo Marino, for his assistance with the intraoperative lens exchange.
{{EXTENDED_NOTES}}
For outcome benchmarking, see the International Glaucoma Surgery Registry.
Scleromalacia management overview — American Academy of Ophthalmology