Overview
This video reviews the defining clinical features of Fuchs’ Uveitis Syndrome, from its characteristic heterochromia and stellate keratic precipitates to the fine vessels crossing the trabecular meshwork. Professor Keith Barton highlights the diagnostic subtleties that distinguish Fuchs’ from other causes of iris pigment loss, as well as its frequent association with secondary open-angle glaucoma. The discussion also addresses management considerations, including cautious steroid use and surgical intervention when required.
Video on YouTube
Fuchs Uveitis Syndrome presents with heterochromia, stellate keratic precipitates, and a risk of secondary open-angle glaucoma.

If age-restricted, please watch this video directly on YouTube.
Key points
- Fuchs’ Uveitis Syndrome presents with diffuse stellate keratic precipitates and iris heterochromia.
- Loss of iris pigment and fine vessels in the trabecular meshwork are characteristic findings.
- Posterior synechiae are typically absent, despite chronic inflammation.
- Secondary open-angle glaucoma is frequent and often resistant to medical therapy.
- Topical steroids should be used selectively, as they may exacerbate intraocular pressure elevation.
Transcript
Fuchs Uveitis Syndrome: Clinical Features
Fuchs’ Uveitis Syndrome, or Fuchs’ Heterochromic Cyclitis, has traditionally been characterised by iris heterochromia and keratic precipitates that are typically evenly spaced over the entire corneal endothelial surface. These precipitates are often stellate in shape with fine interconnecting spindles, as can be seen here [00:25].
Long-standing keratic precipitates may become pigmented and sometimes produce an impressive appearance on gonioscopy. However, the clinical features of Fuchs’ vary extensively, and careful clinical examination is essential to make the diagnosis.
Read more
Fuchs’ Uveitis Syndrome is a chronic, typically unilateral condition characterised by heterochromia, diffuse keratic precipitates, and absence of posterior synechiae. The iris may show pigment loss, fine vessels, or nodules depending on iris colour. Vitreous opacities and secondary glaucoma are frequent complications, often requiring surgical intervention. Routine steroid therapy should be used cautiously, as it can worsen intraocular pressure control.
Iris Changes and Heterochromia
The iris changes that result in heterochromia may be dramatic, such as loss of the posterior iris pigment layer. This is seen in blue and green irides, often with a transparent membrane around the whole circumference of the pupil margin. The transparent membrane can be seen in this case [01:10] and again here.
Despite chronic inflammation and a pupillary membrane, the pupil still reacts, and posterior synechiae do not develop. Iris transillumination in Fuchs’ contrasts with the classical appearance of pigment dispersion syndrome. When transillumination occurs in severe iritis, it is often accompanied by iris sphincter damage, whereas the sphincter is usually spared in Fuchs’.
Diagnostic Clues and Gonioscopic Findings
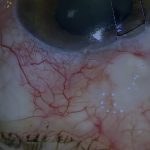
Fuchs’ is the only condition, in my experience, that regularly results in a pigment-free trabecular meshwork, making it easier to see the unique, usually solitary vessels that cross the trabecular meshwork [02:20]. When visible, these are virtually pathognomonic of Fuchs’. Rarely, and usually in more inflamed eyes, multiple vessels are seen crossing the angle circumferentially as well as radially.
Iris Surface Vessels and Stromal Changes
In lighter-coloured irides, fine abnormal vessels may be seen crossing the iris surface [03:16]. The heterochromic effect results from loss of anterior iris stroma in the affected eye, and in dark-coloured irides, nodules are often seen in a regularly ordered circumferential pattern.
Vitreous Opacities and Secondary Glaucoma
Dramatic floaters are often the earliest symptom of Fuchs’, usually predating cataract and glaucoma. Secondary open-angle glaucoma is common, typically resistant to medical therapy and often requiring surgery. It is critical to recognise the glaucoma risk when managing cataract or vitreous opacities.
Management Considerations
Topical steroid treatment can worsen glaucoma. While occasionally useful, for example with intraocular lens deposits, steroids should not be used routinely to treat flare and cells, as they have no long-term proven benefit in Fuchs’ [05:34].
For outcome benchmarking, see the International Glaucoma Surgery Registry.
For more information on Fuchs Heterochromic Iridocyclitis, visit EyeWiki.