Overview
Paul Glaucoma Implant exposure repair is demonstrated here using sulcus repositioning, tight scleral fixation, and amniotic membrane closure in an eye with limited conjunctiva. This detailed step-by-step video highlights key surgical considerations for reducing re-erosion risk when primary conjunctival closure is not possible.
Video on YouTube
Paul Glaucoma Implant exposure repair using sulcus tube repositioning, tight scleral fixation and amniotic membrane closure to reduce re-erosion risk.

If age-restricted, please watch this video directly on YouTube.
Key points
- Reposition the tube posteriorly via a sulcus entry to shorten the external course and reduce re-erosion risk.
- Secure the tube to sclera with tight mattress sutures and cover with a broad scleral patch graft.
- Use amniotic membrane when conjunctiva is insufficient; orient epithelial side up and tuck under adjacent conjunctiva.
- Undermine especially at the limbus to prevent epithelialisation beneath the membrane and promote integration.
- Expect gradual epithelialisation over weeks to months; fibrin glue stabilises the membrane during meticulous suturing.
Transcript
The video demonstrates a tube exposure repair procedure in an eye with limited conjunctival mobility following a Paul Glaucoma Implant. Tube exposure repairs are not uncommon, but in this case, the exposure occurred only a few months after the original surgery. The initial operation had been complicated by a very tight conjunctival closure, requiring the assistance of a senior surgeon. As a result, the conjunctiva was under considerable tension and subsequently exposed.
Paul Glaucoma Implant Exposure Repair
When repairing an exposed tube, it is standard practice to reposition the tube more posteriorly to shorten the external course, reducing the likelihood of re-erosion, and to patch or re-tunnel the tube. In this case, however, there was insufficient conjunctiva for closure, so additional tissue was required. Rather than taking an autograft from the fellow eye, amniotic membrane transplantation was selected as a simpler and effective alternative. Since Don Budenz and I first described amniotic membrane transplantation for glaucoma surgery in the late 1990s, several methods have been published. The technique I demonstrate here is one I have used for over 25 years and has proven to be a reliable solution when no conjunctiva is available for closure.
Read more
{{EXTENDED_NOTES}}
Surgical Overview
This video illustrates how I repaired an exposed glaucoma drainage device where there was minimal conjunctiva for closure, and how amniotic membrane transplantation was used to assist in the repair. Shunt implants carry a small long-term risk of tube erosion through overlying conjunctiva, even when patched.
In this case, the Paul Glaucoma Implant eroded approximately six months after implantation—an unusual occurrence. Operative notes indicated that conjunctival closure had been difficult at the time of implantation due to a tight palpebral aperture and conjunctiva. The eye had a background of primary angle-closure glaucoma treated with laser iridotomy, a branch retinal vein occlusion with panretinal photocoagulation, and a phaco–intraocular lens procedure, but no previous conjunctival surgery. There was no history of conjunctival disease or intolerance to topical medication.
The conjunctiva was carefully reopened, preserving as much tissue as possible. The intention was to close the defect using amniotic membrane, without which closure would likely be impossible. The tube was to be repositioned more posteriorly into the sulcus to shorten its external course and reduce the risk of further erosion.
Tube Repositioning and Trimming [03:10]
A useful technique is to enter via the sulcus but advance the tube through a small hole in the iris so that the tip lies in the anterior chamber. This can be achieved by advancing a 25-gauge needle from the sulcus through the iris and into the anterior chamber. Getting the tube to follow the needle tract often requires several attempts.
The tube was withdrawn from its original entry site and inserted through the new one. Fortunately, the previous entry site did not appear to be leaking and did not require immediate plugging. The tube passed through the needle iridotomy on the first attempt, but it was initially too long and needed trimming. After shortening, it lay well on the anterior iris surface. Further minor trimming achieved an ideal length and position.
To ensure the old entry site was watertight, a scleral “bung” fashioned from donor sclera was secured with fibrin glue.
Scleral Patch Graft and Tube Fixation [06:30]
Before patching, the tube was fixed securely to the sclera with 9-0 nylon mattress sutures, ensuring knots were not positioned over the tube. I typically use two, occasionally three, mattress sutures. Fixing the tube tightly eliminates any movement, which reduces the likelihood of future erosion. Tubes that indent the sclera, especially near the limbus, tend to erode less often.
A wide donor scleral patch graft was then placed to cover the tube and minimise future exposure risk. Because of the poor conjunctiva and Tenon’s capsule, a larger patch than usual was chosen. It was secured in place with fibrin glue.
Amniotic Membrane Transplantation [08:20]
Since there was insufficient conjunctiva for either primary closure or an autograft, an amniotic membrane was used. For the membrane to epithelialise and integrate, surrounding epithelium must be able to migrate over it. This is achieved by tucking the membrane beneath the adjacent conjunctiva on all sides, including along the corneal margin.
A crescent blade was used to release conjunctiva where it adhered to the sclera. Undermining the surrounding tissue is essential; otherwise, the amnion will fail to integrate. In particular, undermining the limbus is critical—if not done, the sclera can epithelialise underneath, preventing integration and causing the membrane to slough off. Tucking promotes gradual epithelialisation over the amnion, which ultimately becomes integrated and protects the underlying graft.
The amniotic membrane acts as a continuous basement membrane for epithelialisation, shielding the patch graft beneath and reducing melting or further erosion. The membrane must be oriented correctly with the epithelial side facing upward and is trimmed slightly larger than the defect. It is tucked into the limbal groove and around the perimeter with an iris repositor, assisted by fibrin glue to hold it in place while sutures are applied.
Securing the Membrane [10:50]
Once positioned, the membrane was anchored at each corner using 10-0 nylon sutures, with multiple passes drawing it into the groove. This process is slow and meticulous, often taking two hours or more. Fibrin glue has significantly improved the procedure’s ease and stability, preventing the membrane from slipping during suturing.
Further fixation was achieved by placing additional 10-0 nylon sutures at the limbus, pulling the membrane securely into place. Each edge was then sutured beneath the adjacent conjunctival margin using a locked continuous 10-0 Vicryl suture, which was tied off periodically until the membrane was firmly secured.
Post-Operative Course [13:30]
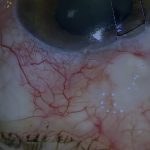
On the first postoperative day, the tube was well covered, the amniotic membrane intact, and the tube well positioned on the iris surface. At day eight, the appearance remained stable. Because the membrane is transparent, it can be difficult to visualise postoperatively, sometimes leading to mistaken claims that it has disappeared. In this case, it was clearly visible between the patch graft and the limbus.
Complete epithelialisation may take several weeks or months. At five weeks, the membrane was partially but actively epithelialising. At two months, there remained a small defect with noticeable vascular ingrowth, which progressed further by three months with only a minor residual epithelial gap.
Summary and References [15:50]
This video demonstrates how a tube can be repositioned via a sulcus entry site to shorten the external course and reduce re-erosion, and how amniotic membrane transplantation can be employed effectively when no viable conjunctiva is available locally or for autograft. References are provided for the first reports of amniotic membrane use in ophthalmology in the 1990s and our early publications on its application in glaucoma surgery.
For outcome benchmarking, see the International Glaucoma Surgery Registry.